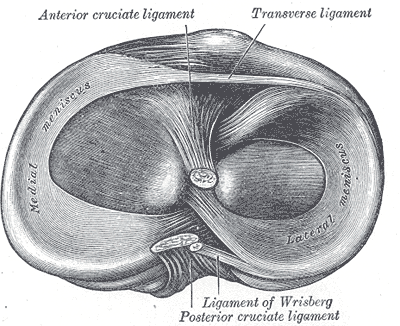

Sitting between the femur bone of the thigh and the tibia of the shin are the meniscus, made of cartilage and designed to help absorb and distribute shock and also stabilize the knee during movement. There are a number of menisci in the body though most people automatically think of the knee when they hear mention of the word meniscus. The two menisci of the knee sit laterally (outside) and medially (inside).
Cartilage is a malleable connective tissue often found in the joints between bones. Though it is softer than bone, it is harder and less flexible than muscle. The elasticity of the meniscus, minimal as it might be, helps to balance and stabilize the knee. With each movement of the knee—flexion, extension, minimal rotation— the meniscus change shape to accommodate the movement of the joint.
One of most common orthopedic surgeries is to repair tears in the meniscus of the knee. As we get older there is less blood flow to the meniscus and since blood to essential to all healing, the lack of blood flow makes the meniscus more susceptible to injury.
Most meniscus injuries occur through a planting and twisting action. My first meniscus injury—set up by too much hyperextension—came during a softball game where I set my foot to pivot and while the knee turned the foot did not, resulting in a mini explosion in my knee.
When you hear the phrase torn cartilage the reference is almost always to the meniscus of the knee and surgery is often the choice people make for repair. Tears of the meniscus can take many forms in varying degree and arthroscopic surgery can get into the joint and clean those pesky problems up.
The question is whether those tears need to be repaired. In the case of the first of three knee surgeries that I underwent, the lateral meniscus was torn completely off its mooring and was reconnected. This is a more complicated procedure and requires way more time to heal.
When it comes to the more basic cleanouts— I had two of those as well—while the surgery is fairly routine I am not sure it is always necessary. For one, without a baseline MRI to use as a reference point, a doctor really has no idea when the tear he sees on the film occurred. Without that knowledge it is hard to make the correct decision about whether a surgical procedure is warranted.
Many years later I don’t regret having the surgeries that I had. I have no knee pain and I don’t limit my activities in any way. Also, the arthritis that I was told to expect to creep into the joint has not begun. But at the same time I have worked with numerous people who had meniscus cleanouts recommended and watched their pain dissolve through changing movement patterns and an exercise protocol.
***